


































Daudi O. Simba (MD, PhD) is Associate Professor at Muhimbili University of Health and Allied Sciences (MUHAS) in Tanzania. He is one of the innovators we support in our Stars In Global Health program, for a project aiming to improve access to anti-malarials
World Malaria Day (April 25) is a chance to shine the spotlight on the global effort to fight malaria. Raising awareness remains critically important. About 3.2 billion people – that is almost half of the world’s population – are at risk of malaria. In 2013, there were about 198 million malaria cases and an estimated 584,000 malaria deaths (WHO data). The numbers show that the overwhelming majority of these deaths occur in Africa, South of the Sahara. Furthermore, over 80% of mortal malaria cases occur among children under five. Although malaria infection has declined substantially from 2000 (26%) to 2013 (14%), there is another, troublesome trend that deserves attention: household data shows that between 2011 and 2013, over half of feverish children treated for malaria did not receive the recommended treatment, which is artemisinin-based combined therapy. Paradoxically, the malaria burden seems to follow the ‘inverse care law’ that states that the availability of good medical care tends to vary inversely with the need for the population served (Hart 1971). As a result, children in rural remote areas in Tanzania have the highest burden of malaria, yet they are left with the least access to services (Simba et al, 2010).

In recent years, a lot of efforts have been made to increase access to health services in rural areas, including treatment of malaria. One example is the country-wide introduction of the Accredited Drug Dispensing Outlets (ADDO), drug shops that are allowed to sell a selected number of prescription-only medicines after a short training to the dispensers. The challenge however remains that most of the ADDOs are located in semi-urban and geographically accessible areas where the outlet owners have a guaranteed profit margin due to the concentration of people. Rural remote areas see none or very sparse ADDOs because the outlets wouldn’t be economically sustainable due to low purchasing power and scattered population. As a result, sick children in more remote areas still fail to have prompt access (within 24 hours) to these facilities and life-saving drugs (Simba et al, 2010).
Combining Motorcycles and Drug Outlets
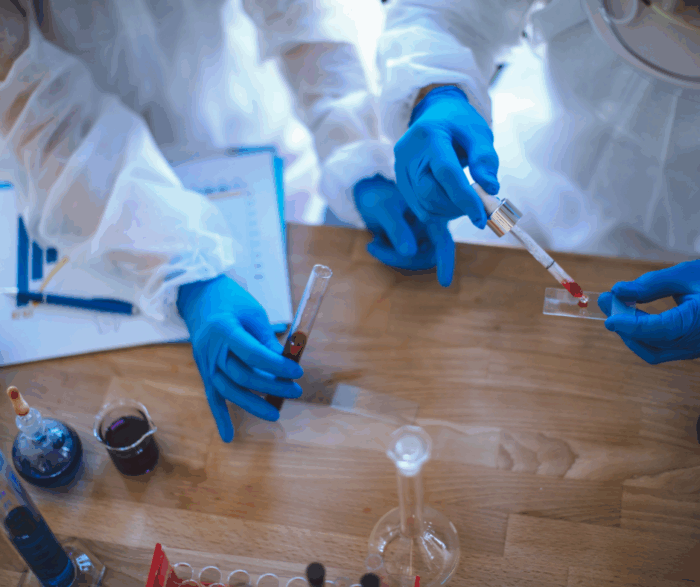
In 2013, Grand Challenges Canada (funded by the Government of Canada) supported The Malaria Drugs on the Wheel Project with a seed grant in the Stars In Global Health program. The project was conducted through Muhimbili University of Health and Allied Sciences (MUHAS) and aimed to increase prompt access to malaria rapid diagnostic test and treatment drugs. The overarching idea was to provide antimalarials called artemether-lumefantrine (ALu) to those who tested positive for malaria. People who tested negative or showed signs of severe symptoms, would be referred to a health facility.
This innovative strategy combined the country-wide implementation of the ADDOs with the booming motorcycle transport business in Tanzania.The latter, known as bodaboda, has dramatically improved physical access to products and services in many areas, including rural villages. The ideas was to leverage this fast growing motorcycle sector in Tanzania to expedite access to effective antimalarials through the ADDO strategy, to reach rural remote areas, where the disease burden is high and purchasing power is low. On one hand, private ADDO owners who showed interest in joining the project, and who had access to motorcycles, were engaged. On the other hand, the plan also involved the recruitment of existing Community Health Workers (CHWs) and other rural based entrepreneurs who qualify as candidates for ADDO training, in villages located 5 km or more from a nearby health facility or an ADDO. The CHW’s were provided a small profit margin as an incentive to motivate them for rendering services. These CHWs proved crucial to link ADDOs with the caretakers of sick children.
Access to malaria diagnosis and treatment improved
The Malaria Drugs on the Wheels Project was able reach and provide diagnostic and treatment services to all remote villages in Masanze ward in Kilosa district. While prompt access to malaria diagnosis and treatment was more or less similar between intervention and control areas prior to the intervention, the prompt access increased after the intervention, from 65.5% to 88.1%.

Extensive discussion with CHWs revealed that, unlike in the past, they observed no under-five deaths associated with fever during the 12-month study period. Caretakers also expressed a high level of satisfaction with the availability and provision of services.
The study also revealed that even within a rural area, there are people who are more marginalized than others. This group usually resides in hard to reach areas that include villages in hilly and mountainous areas, or settlements that are waterlogged during rainy season. These areas can not even be reached by motorcycles and need to be looked at with a different methodology.
Overall, combining the ADDOs and the mushrooming motorcycle transport business can help to ensure that antimalarials reach the neediest; thus attaining the dream “Tanzania without malaria deaths is possible.”
We encourage you to post your questions and comments about this blog post on our Facebook page Grand Challenges Canada and on Twitter @gchallenges.