Project Lead(s): Mohamed Mohamed
Issue
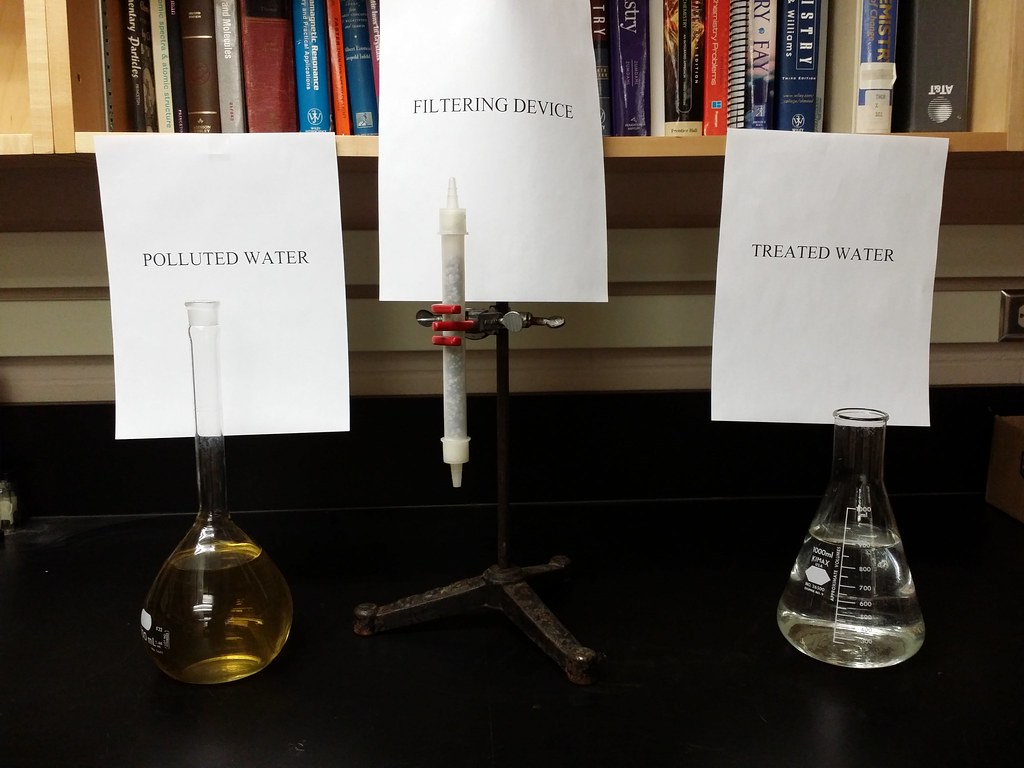
Arsenic in drinking water threatens many communities worldwide and, in Bangladesh, close to 57 million people suffer from arsenicosis through arsenic-contaminated drinking water in what the World Health Organization has called the world’s worst mass poisoning.
Removal of arsenic from the water provides only a partial solution, as it cannot address prior exposure, nor can it address arsenic from crops irrigated with contaminated water.
Solution
This project sought to investigate whether oral selenium can remove the arsenic from sufferers of arsenic exposure, by conducting a Phase I/II clinical trial in Bangladesh.
Over a period of 10 days, a total of 40 volunteer arsenicosis sufferers were housed in a local private in-patient clinic.
While in the clinic, they followed a fixed, communal diet consisting of drinking water and meals from their village. On the sixth day in the clinic investigators supplied them with a single dose of either placebo (table salt, 0.8 mg) or anhydrous sodium selenite (table salt containing 0.8 mg selenium) labelled with a non-radioactive, naturally occurring isotope (77Se), to distinguish it from selenium already in the body.
Pre- and post-analysis of arsenic and selenium levels in feces, urine and blood samples would be undertaken.
In addition, the research team evaluated stable formulations of both iodine and selenium in table salt, as part of a project to deploy double-fortified table salt.
Samples of six different commercial iodized table salts from Bangladesh were tested and were analyzed, both for total iodine and speciation. Formulations of table salt with different selenium compounds were tested under conditions of prolonged exposure to heat and humidity, and for both selenium and iodine speciation.
In all the formulations that were tested, no changes in chemical forms of selenium and iodine were detected, confirming the proof-of-concept for this aspect of the work
Outcome
The analyses of all samples in the trial has not yet been completed.
Preliminary analyses of some of the fecal samples revealed a rather unexpected finding: that fecal arsenic varies substantially between individuals – by nearly an order of magnitude – despite the fact that all individuals consumed similar levels of arsenic as part of their normal daily diets.
One of the most perplexing facts about arsenicosis is that it affects only some individuals in a community, with others remaining relatively healthy, while all are consuming essentially the same food and water. The finding of the substantial variation in arsenic fecal excretion may be important in understanding why arsenicosis affects only some and not others in a given community.
The team hypothesizes that those who retain arsenic may be more likely to show more severe arsenicosis progression than those who excrete more, due to variation in the gut microbiome.
This revelation has led the team to initiate a new study, in collaboration with Professor Joanne Santini of University College London, to investigate this theory.
The decision to apply for Transition To Scale (TTS) funding will be made when the final analyses are complete.